
Chronic Pelvic Pain Syndrome(CPPS)
I’ve been thinking of sharing this topic for a long time, because unlike most of my female clients, males tend not to seek for health providers actively to talk about their concerns.
Prostatitis-related conditions are the most commonly diagnosed urological issue in men under the age of 50, manifesting in symptoms such as pelvic pain, bladder and sexual dysfunction, and psychological issues.
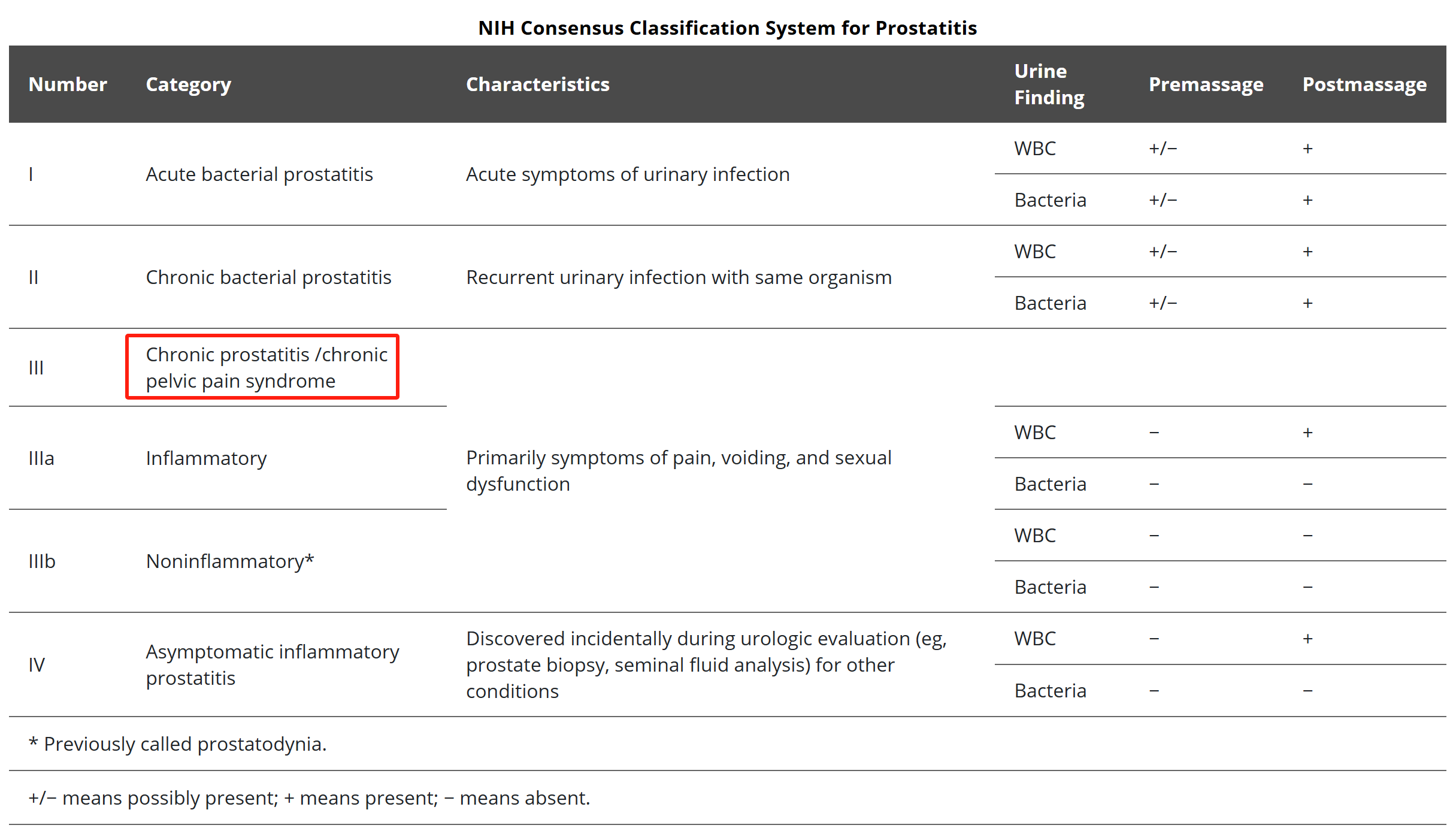
Sometimes prostatitis is due to a bacterial infection, however, 90-95% of cases are considered non-bacterial and fall under the Chronic Pelvic Pain Syndrome (CPPS) category [1,2], a more befitting name to the correct diagnoses of pelvic pain.

Most of CPPS patients have at least two or more symptoms listed as below,
Urinary Frequency / Urgency / Hesitancy
Pain or Relief After Bowel Movement
Pain with Sitting, lower Abdominal Pain
Rectal / Perineum Pain
Pain During or After Sex
Sexual dysfunction (Premature Ejaculation, Erectile dysfunction, Painful ejaculation)
Tailbone / Low Back Pain
Depression / Anxiety About Symptoms
The Diagnosis
Research reveals it can take men with pelvic pain up to 7 years to get an accurate diagnosis[3]. Doctors give a number of names depending on what subspecialty of doctor you see. Among them are: prostatitis, chronic proctalgia, levator syndrome/spasm, pelvic floor dysfunction, coccydynia, pudendal neuralgia, chronic proctalgia, puborectalis syndrome, piriformis syndrome.
The CPPS patients I have met all have similar pasts: they have seen the urologists, had examinations and taken different types of medications for prostatitis, but their symptoms got back a week or two. Conventional medical treatments can at best provide partial or short-term relief; surgical interventions or injections may even make it worse.
What’s the solution?
Before we get to the answer, we as health providers and patients themselves need to be aware that chronic pelvic pain syndrome is both a systemic and local problem.
Q: Why is it systemic?
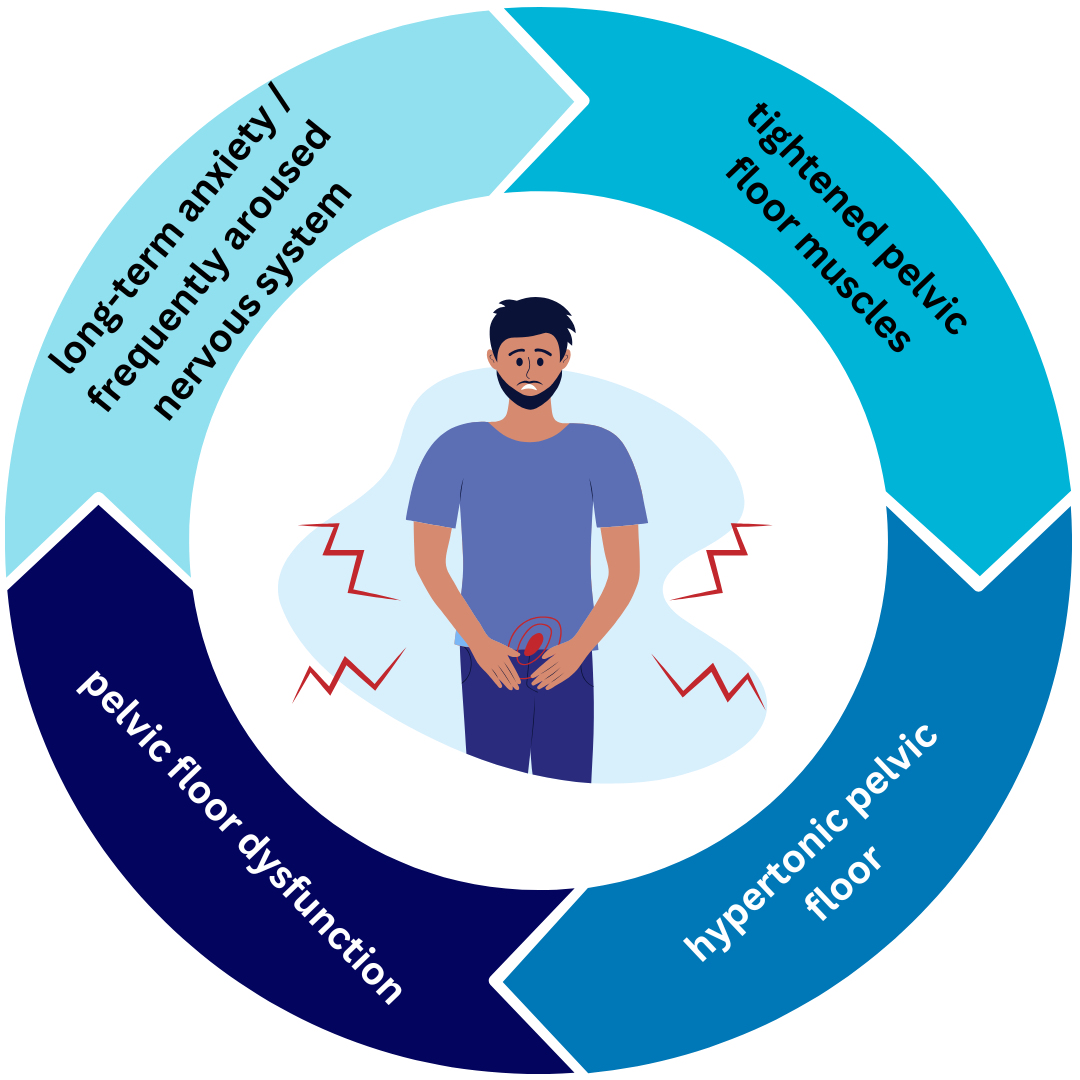
A: When the nervous system is typically frequently aroused, the pelvic muscles get tightened chronically.
Q: And why is it local?
A: Taking the example from mammals, when an animal is afraid, the muscles of the pelvis tighten, pulling in the tail. While humans no longer have a tail, the pelvic muscles still tighten up in certain individuals who chronically deal with stress. This chronic contraction/ spasm in the pelvic floor can cause chronic pain from the area above the pubic bone, through the penis, testicles, perineum, anus, tailbone and low back. This chronic contraction can result in problems with urination, defecation, ejaculation, sitting, and other basic day-to-day functions.
The CPPS patients will only get better if we address both problems from a holistic perspective. Giving the fact that the source of CPPS symptoms is resulting from pelvic floor muscles instead of prostate, neither antibiotics nor anti-inflammatories can eliminate these symptoms.
What’s the treatment?
When pelvic floor physical therapists evaluate the patients who were previously diagnosed with CPPS, trigger points in pelvic floor muscles and related muscles are identified.
Since we now realize long-term anxiety and frequently aroused nervous system will tighten the pelvic floor muscles, accumulated with time then become painful and dysfunctional chronically.
Pelvic floor physical therapy is an effective treatment for CPPS, not only it helps to eliminate the symptoms but also build up the confidence for patients and improve their quality of life. Pelvic floor physical therapy includes,
Adjusting pelvic floor muscle tone (manual therapy, MFD),
Strength / relaxation training (neural control training, yoga, meditation),
Overall adjustment of the pelvic girdle (sacroiliac joints, hip joints, lumbar spine),
Breathing training (coordination of pelvic floor and diaphragm).
As a pelvic floor PT, I feel honored to work with each individual, and it is really my passion to support all genders with pains and dysfunctions with my knowledge and experience. If you are diagnosed with CPPS, or wondering what you’re experiencing at the moment could be CPPS, click the button below and get in touch today!
References
1. Magistro G., Wagenlehner F.M.E., Grabe M., Weidner W., Stief C.G., Nickel J.C. Contemporary Management of Chronic Prostatitis/Chronic Pelvic Pain Syndrome. Eur. Urol. 2016;69:286–297. doi: 10.1016/j.eururo.2015.08.061.
2. Lipsky B.A., Byren I., Hoey C.T. Treatment of Bacterial Prostatitis. Clin. Infect. Dis. 2010;50:1641–1652. doi: 10.1086/652861.
3. McNaughton Collins M, Pontari MA, O’Leary MP, Calhoun EA, Santanna J, Landis JR, et al. Quality of life is impaired in men with chronic prostatitis: The Chronic Prostatitis Collaborative Research Network. J Gen Intern Med. 2001;16:656–62. doi: 10.1111/j.1525-1497.2001.01223.x.