
Why Kegels Don’t Always Work — It’s Not Just About the Muscles
Kegel exercises are widely recommended for improving pelvic floor health. Many people faithfully perform them every day, expecting better bladder control, reduced pelvic symptoms, or improved core stability.
Yet a common question arises in pelvic floor physical therapy clinics:
“I’ve been doing Kegels regularly—why aren’t I seeing much improvement?”
The answer may surprise you.
Emerging research suggests that pelvic floor training is not simply about strengthening muscles. Instead, it involves a complex interaction between the brain, nerves, and muscles. In other words, effective pelvic floor rehabilitation is as much about training the nervous system as it is about building muscle strength.
Understanding this concept can help explain why Kegel exercises alone sometimes fall short—and why guided pelvic floor physical therapy can make a significant difference.
The Pelvic Floor: A Brain–Muscle System
All voluntary muscle activity in the human body is controlled by the brain. The pelvic floor is no exception.
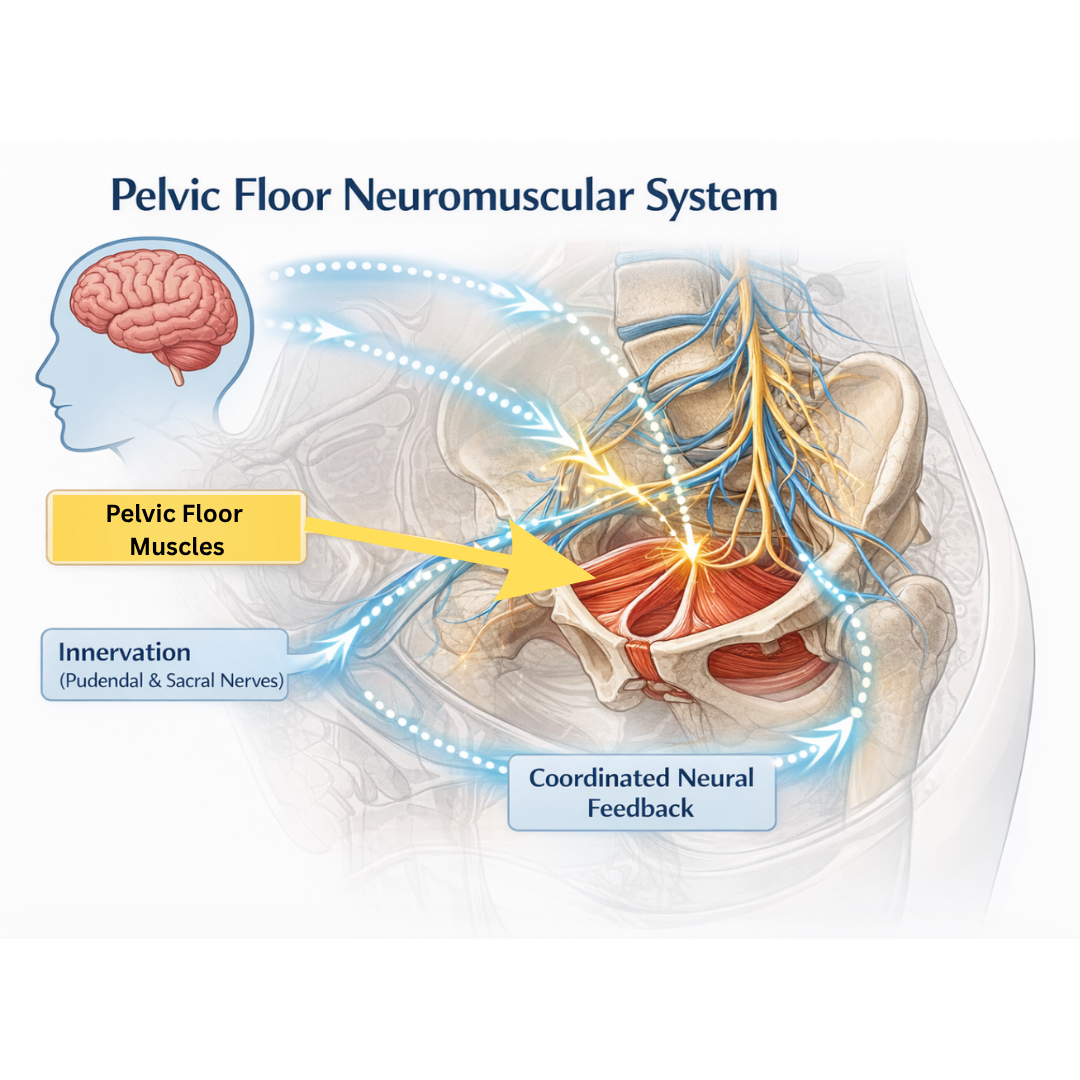
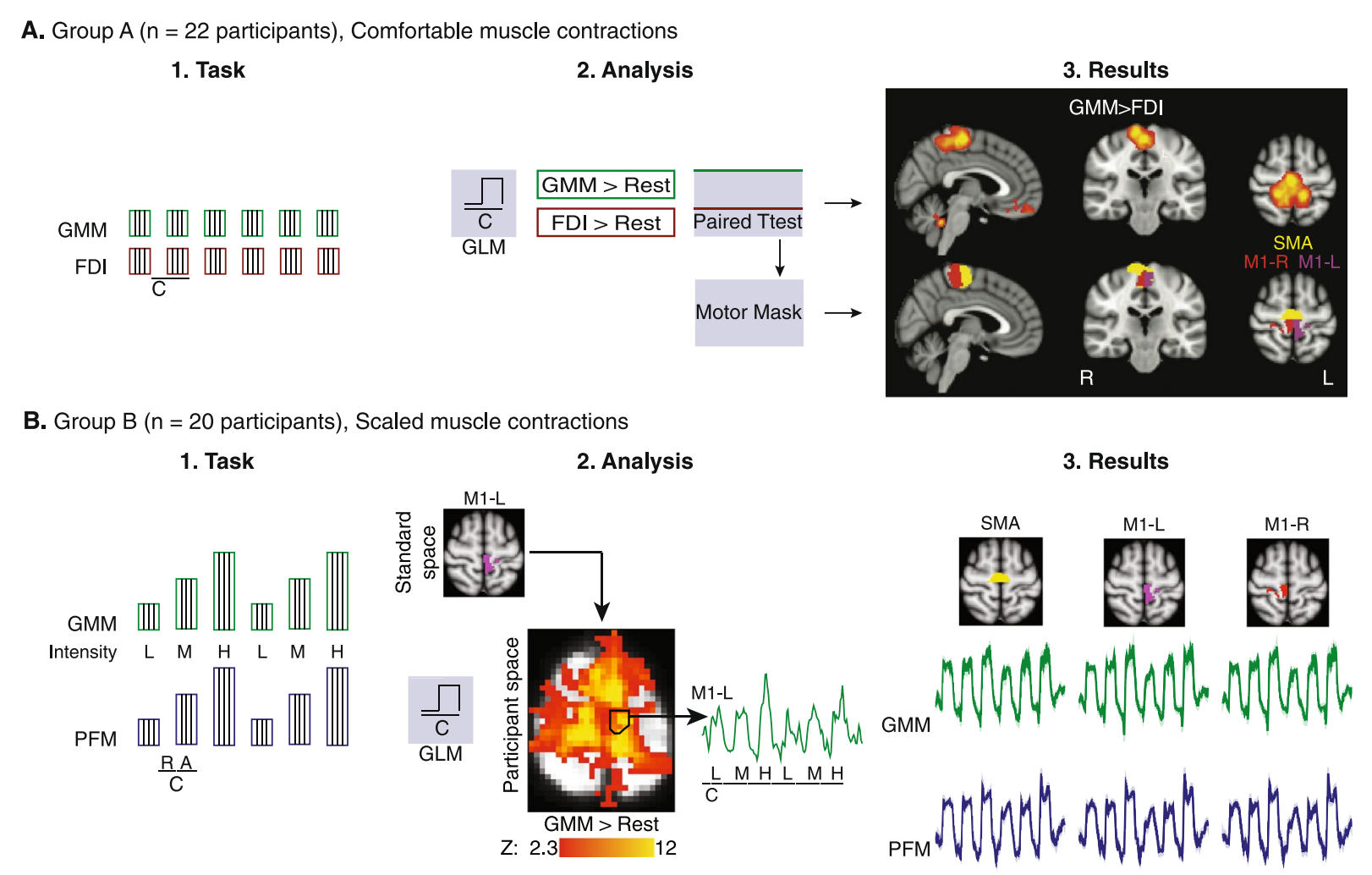
A 2018 study published in Scientific Reports explored how the brain controls pelvic floor muscle activity. Researchers used several advanced tools, including:
Electromyography (EMG) to measure muscle activation
Functional MRI (fMRI) to observe brain activity
Transcranial magnetic stimulation (TMS) to examine neural pathways
The results provided important insights for pelvic floor rehabilitation.
First, the pelvic floor muscles can be activated through different functional patterns.
Second, their control in the brain involves multiple interconnected regions, rather than a single control center.
These findings reinforce an important idea: pelvic floor function depends on a coordinated neuromuscular system.
Two Functional Activation Patterns
The study identified two primary ways the pelvic floor muscles are activated.
1. Isolated Pelvic Floor Contraction
This pattern is familiar to most people. It occurs during Kegel exercises, when individuals intentionally contract the pelvic floor muscles.
Isolated pelvic floor activation is also used in:
pelvic floor rehabilitation training
voluntary control of urination
certain therapeutic exercises
In this situation, the pelvic floor muscles can contract independently of surrounding muscles, such as the gluteal muscles.
2. Functional Synergy With the Gluteal Muscles
In everyday movement, however, the pelvic floor rarely works in isolation.
During activities such as:
coughing
running
lifting heavy objects
the pelvic floor muscles typically activate together with the gluteus maximus.
This coordinated activation helps regulate intra-abdominal pressure and contributes to overall core stability.
Interestingly, the study found that these muscles have different neural activation thresholds.
The pelvic floor muscles require less neural input to activate, meaning they tend to engage more easily. The gluteal muscles require stronger neural signals.
As a result, the pelvic floor muscles usually activate slightly earlier—about 140 milliseconds before the gluteal muscles.
This timing suggests that the pelvic floor plays a key role in preparing the body for movement and stabilizing the core.
Pelvic Floor Control Is Distributed in the Brain
For many years, pelvic floor movement was believed to be primarily controlled by the Supplementary Motor Area (SMA) in the brain.
However, modern neuroimaging studies show that control is actually more complex.
Pelvic floor activation involves a network of brain regions, including:
the Supplementary Motor Area (SMA)
the Primary Motor Cortex (M1)
Rather than relying on a single control center, pelvic floor movement is governed by a distributed neural network.
This network allows the brain to coordinate pelvic floor activity with breathing, posture, and movement.
What This Means for Pelvic Floor Rehabilitation
In clinical practice, many patients become discouraged when they don’t see quick results from exercises.
But pelvic floor rehabilitation is not simply about making a muscle stronger. It also requires the nervous system to learn how to recruit and coordinate those muscles efficiently.
Pelvic floor physical therapy therefore focuses on more than strength training. Treatment may aim to:
improve neuromuscular coordination
restore healthy movement patterns
enhance muscle recruitment and timing
optimize functional integration with the core
Over time, the brain gradually adapts and develops more efficient control strategies.
This adaptive process is known as neuroplasticity—the brain’s ability to reorganize and refine its neural pathways.

Why Guided Pelvic Floor PT Often Produces Better Results
In conditions such as urinary incontinence and chronic pelvic pain, research suggests that the brain’s control of the pelvic floor may already be altered.
These changes may include:
differences in motor cortex connectivity
structural changes in gray matter
altered brain–bladder communication pathways
Because of these neurological changes, restoring pelvic floor function often requires more than simple exercise repetition.
Effective rehabilitation may involve:
motor retraining
neuromuscular coordination
sensory feedback
progressive functional training
This is why structured pelvic floor physical therapy frequently leads to better outcomes than unsupervised exercise alone.
The Takeaway
Kegel exercises can be helpful—but they represent only one piece of the puzzle.
Pelvic floor health is not just about training a muscle. It is about restoring coordination within a complex brain–muscle system.
When therapy addresses both the neurological control and the muscular function of the pelvic floor, rehabilitation becomes far more effective.
And that is the true goal of modern pelvic floor physical therapy.

参考文献 References
1. Yani MS, Wondolowski JH, Eckel SP, Kulig K, Fisher BE, Gordon JE, Kutch JJ. Distributed representation of pelvic floor muscles in human motor cortex. Sci Rep. 2018 May 8;8(1):7213. doi: 10.1038/s41598-018-25705-0. PMID: 29740105; PMCID: PMC5940845.
Disclaimer: This article reflects the author’s professional opinion and is not a substitute for personal medical advice. The information provided is intended to help readers make informed decisions about their health.