
An Evidence-Based Guide to Diastasis Recti Rehabilitation
If you have ever been pregnant and found that your stomach never quite regains its flatness after giving birth, or if you notice a small ridge bulging in the middle of your abdomen when you exercise – a phenomenon often referred to as "doming" – you may have come across the term diastasis recti abdominis (DRA).
In clinic, we frequently hear questions along these lines:
"People tell me that a few sessions with a machine will close the gap in my abdominal muscles."
"Isn't machine-based treatment more effective than doing exercises?"
With the growth of social media, it has also become increasingly common to see promotional posts from clinics advocating various devices for treating diastasis recti – such as INDIBA, EMS, and electrical stimulation. Perhaps fuelled by market hype, many patients have come to assume that "diastasis recti is a condition that can be fixed simply by using a machine."
But is that really the case?
If we turn to evidence-based medicine, recent international research tells us that the rehabilitation of diastasis recti abdominis is far more complex than that.
Rethinking Diastasis Recti Abdominis
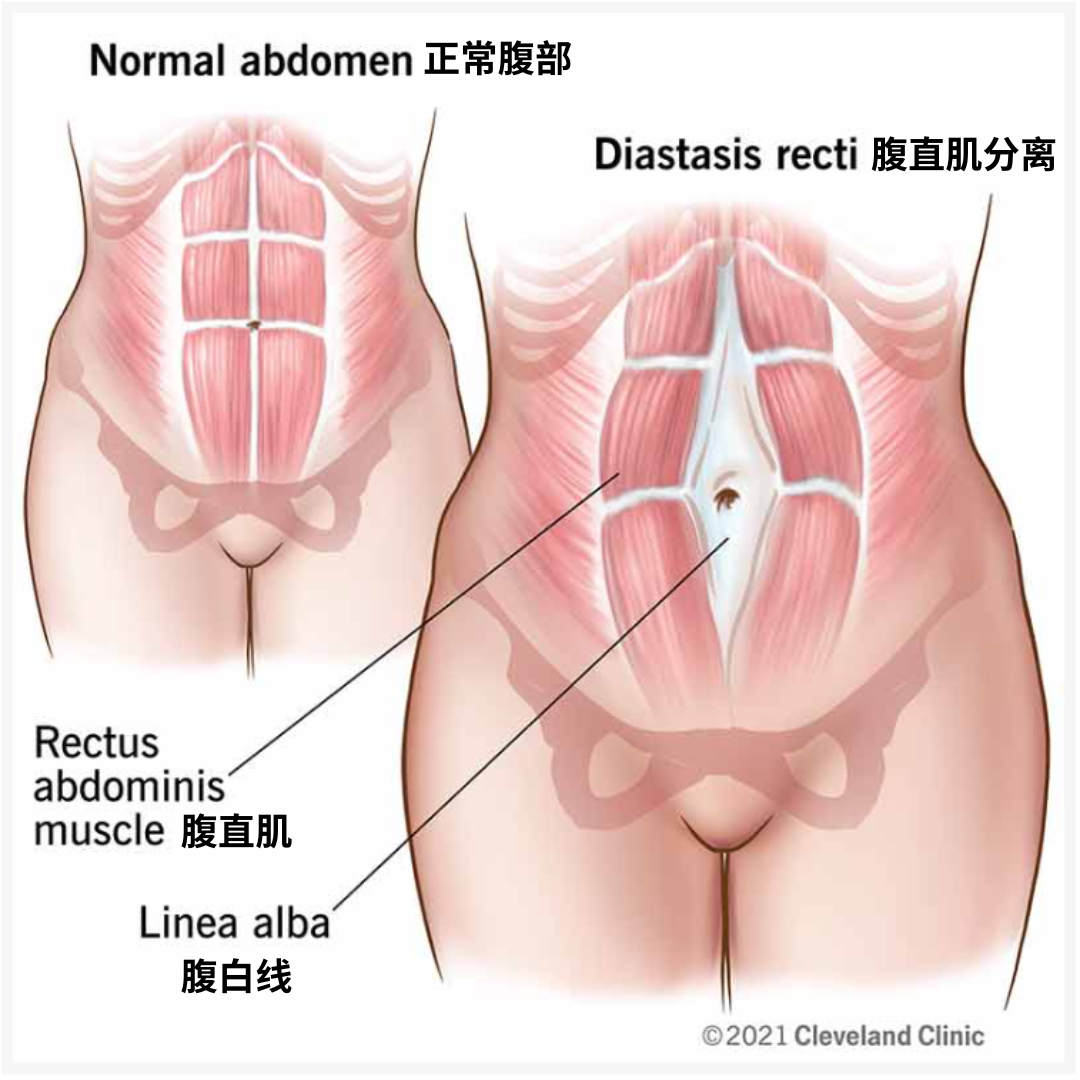
Diastasis recti abdominis refers to an increase in the distance between the two bellies of the rectus abdominis muscle, typically occurring after sustained stretching of the linea alba. The most common contributing factors include pregnancy, multiple pregnancies, macrosomia, twin gestation, and obesity.
Research indicates that the prevalence of diastasis recti in the third trimester can be as high as 66–100% [1]. While most women experience some degree of spontaneous recovery over time, approximately 30–60% still present with a separation of more than 2 cm at six months postpartum, and around 20% may go on to develop chronic dysfunction [2].
Current consensus in Europe and North America regarding the management of DRA is that physical therapy constitutes the first-line conservative treatment [3]. Swedish clinical guidelines explicitly state that physical therapy is the preferred treatment for DRA, and that surgery should only be considered when there is significant functional impairment and after at least six months of standardised core training has proven ineffective.
It is important to recognise that diastasis recti abdominis is not, in itself, a disease. What truly matters is whether it is affecting your function – for example:
Noticeable bulging or doming of the abdomen when getting up from lying down
Aching in the lower back when holding your baby
Urine leakage when coughing, laughing, or lifting heavy objects
A feeling of core "weakness" or instability when running
Persistent outward bulging of the abdomen during planks
These signs often provide a more meaningful indication of whether your core function has recovered than simply measuring the width of the separation alone.
A New Perspective: Don't Focus Solely on the Inter-Recti Distance
Over the past decade or so, much research has centred on the inter-recti distance (IRD) as a key metric. As a result, many patients have come to believe that "once I train my abdominal muscles back to a one-finger width, I will be fully recovered."
In reality, this is a notion that is increasingly being revised by the international academic community!
Studies suggest that linea alba tension may be a better indicator of abdominal wall function than simply measuring the inter-recti distance [4]. The linea alba acts like a tough "tension band" that connects the two sides of the rectus abdominis. Even if there remains some separation between the two muscle bellies, as long as the linea alba can maintain adequate tension during movement and the core musculature can work together effectively, an individual can still achieve good core stability.
The Core Canister:What Really Needs to Be Restored Is "Coordination"
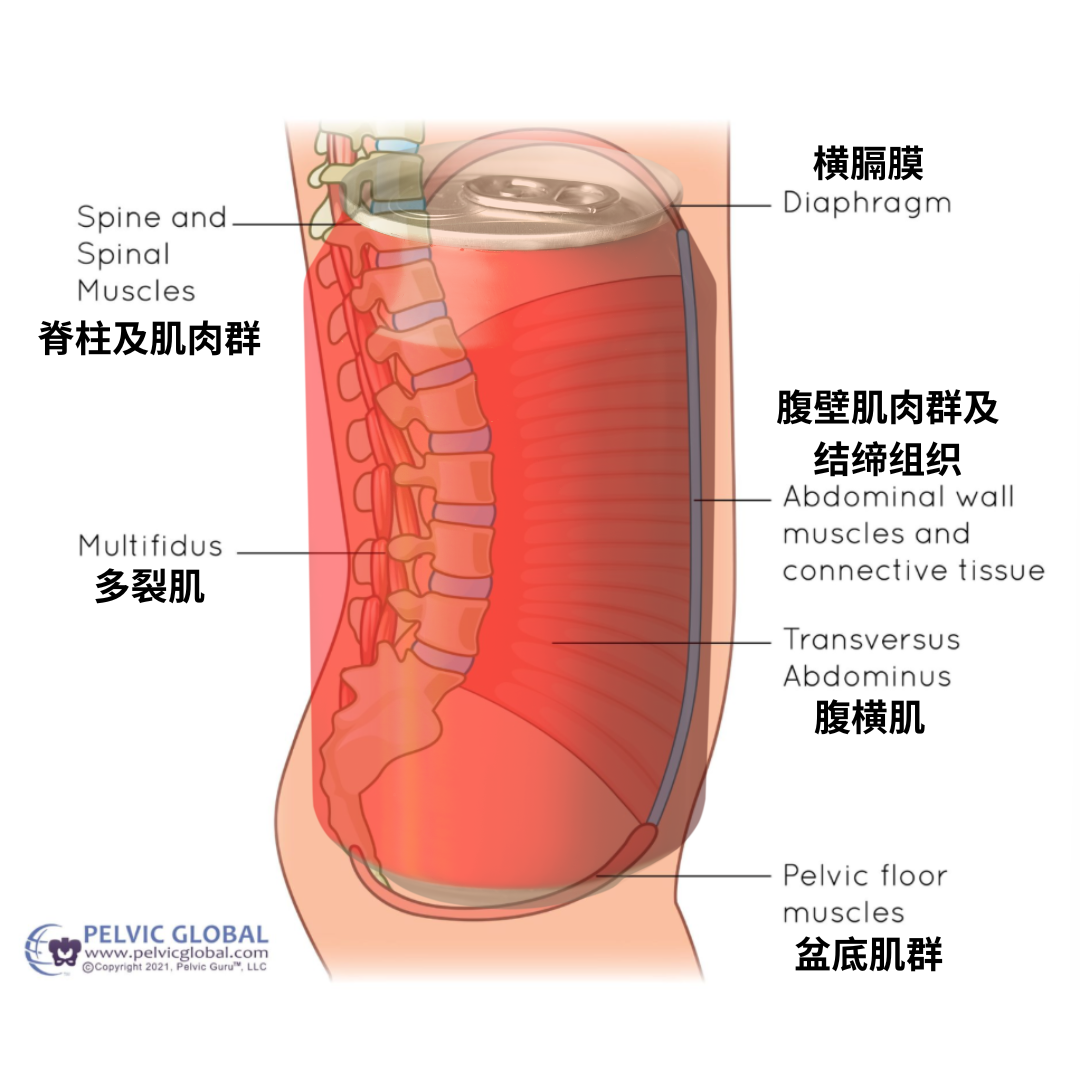
Imagine a soft drink can (see figure):
- The lid is the diaphragm
- The base is the pelvic floor muscles
- The walls are the abdominal wall muscles, including the transversus abdominis, rectus abdominis, and obliques
The core concept of this "can" model is this: intra-abdominal pressure itself does not harm the rectus abdominis. The real issue lies in whether that pressure can be effectively absorbed, distributed, and controlled by the entire core system [5].
If the components of this "can" – top, bottom, and sides – fail to coordinate with one another, then the same amount of intra-abdominal pressure may cause the abdominal wall to bulge forward persistently. This, in turn, increases tension on the linea alba and leaves the patient more susceptible to urine leakage, lower back pain, or diminished athletic performance.
Therefore, the true goal of rehabilitation is no longer to achieve complete closure of the gap between the recti, but rather to restore the abdominal wall's capacity to function as an integrated whole.
What Role Do Devices Play in DRA Rehabilitation?
In the market, numerous clinics and manufacturers promote various devices with claims of effectiveness for treating DRA. One of the devices patients most frequently ask me about is INDIBA – a 448 kHz capacitively coupled resistive radiofrequency (CRRF) technology that is primarily used in clinical practice for pain relief, improving local circulation, and enhancing soft tissue extensibility [6].
To date, high-quality research on conservative management of DRA has predominantly focused on core training, transversus abdominis training, pelvic floor muscle training, and neuromuscular electrical stimulation (NMES). INDIBA has not been featured in major systematic reviews or meta-analyses as a well-evidenced core treatment modality for DRA [6,7].
So what might INDIBA actually help with?
In clinical practice, many postpartum women present not only with diastasis recti but also with concurrent issues such as caesarean scar tightness, abdominal wall pain, and myofascial restrictions. For these specific concerns, INDIBA may serve as a clinically valuable adjunctive tool – helping to raise tissue temperature, alleviate pain, and improve mobility around scar tissue, thereby making it easier for patients to engage in exercise [6].
However, no matter how good an adjunctive tool may be, it cannot automatically teach the body how to breathe, how to control intra-abdominal pressure, how to coordinate the transversus abdominis, or how to restore pelvic floor function. These capabilities still require active training to be regained [4].

Why Physical Therapy Cannot Be Replaced by Devices?
Consider a simple example. If a footballer sustains a ligament injury to the ankle and experiences reduced pain after receiving ultrasound therapy, does that mean they are immediately ready to return to the pitch? Of course not. They still need to rebuild balance, proprioception, muscular endurance, explosive power, running, and change-of-direction ability – among many other things.
The same principle applies to diastasis recti abdominis. Even if pain improves and tissue mobility increases, the body still needs to relearn how to effectively coordinate the entire core system during daily activities and exercise – and how to make rapid adjustments even in moments when intra-abdominal pressure spikes.
What truly rehabilitates you is not the machine itself, but rather the process of re-establishing correct movement patterns after your tissues have improved.
The DocGao Rehabilitation Pyramid: From Breathing to Returning to Sport

Building upon continually evolving evidence-based medicine, we have structured DRA rehabilitation into six distinct levels:
Level One: Comprehensive Assessment
At DocGao, we of course measure the inter-recti distance – but it is merely one item on a much broader assessment. What we truly aim to understand is: Does the diastasis recti actually impose functional limitations? What concerns the patient most? Is there associated urinary incontinence or low back pain? What activities is the patient most eager to return to [8]?
Level Two: Restoring Breathing
Learn to breathe first; then talk about core training. During normal inhalation, the diaphragm descends, the abdominal wall naturally expands, and the pelvic floor undergoes a gentle eccentric movement. During exhalation, these structures coordinately return to a supportive position [5].
If a patient has long been accustomed to breath-holding during exertion, shoulder-breathing, or continuously sucking in their stomach, then even a substantial amount of core training may be compensatory in nature – making it very difficult to establish an effective pressure management system.
Level Three: Pressure Management
Learn to manage intra-abdominal pressure, rather than fear it. Intra-abdominal pressure is, after all, a normal physiological phenomenon [9]. What truly affects abdominal wall function is not the presence of pressure itself, but whether the body can coordinately manage that pressure during movement. The goal of rehabilitation training is to develop movement strategies that can adapt to, distribute, and control pressure.
Level Four: Rebuild Core Coordination
True core stability does not come from sustained contraction of a single muscle, but rather from the automatic adjustment of tension and mutual coordination among many muscle groups in response to movement demands – the diaphragm, transversus abdominis, obliques, multifidus, pelvic floor muscles, gluteals, and hip stabilisers [4].
Contraction of the transversus abdominis (TrA) is a key mechanism for increasing tension in the linea alba and drawing it toward the midline. Therefore, training that targets the transversus abdominis represents a well-established, mechanism-based core strategy in DRA rehabilitation [4].
Level Five: Functional Strength
Strength training is not just for the gym. For postpartum women, what truly needs to be restored is the ability to: lift a child with ease, carry shopping bags, push a pram up a slope, work for extended periods without back pain, and rediscover the sports they once loved. Functional strength training encompasses exercises such as squats, deadlifts, pushing, pulling, carrying, and single-leg stability work [4]. In my clinic, training exercises are practically integrated with everyday moments – incorporating the baby, steps, and prams – to help patients bring their core capacity back into real-life settings.
Level Six: Return to Sport
Returning to sport does not simply mean "if you are pain-free today, you can go and run 10 kilometres." At DocGao, our rehabilitation programme includes a structured Running Protocol to help determine whether a patient's physical condition is ready to resume high-intensity activity:
No significant pain during daily activities
Ability to manage intra-abdominal pressure naturally when coughing, sneezing, or lifting heavy objects
No persistent or significant abdominal doming
No urinary incontinence or pelvic floor symptoms exacerbated by exercise
Ability to perform fundamental strength movements with stability
Restored confidence in one's own body
Only once the patient passes the Running Protocol – receiving the "green light" – does it truly signify that the body is capable of adapting to the high loads and pressures inherent in sport.
In Closing
Your body is not fragile simply because you have given birth. True rehabilitation is not about returning to your pre-pregnancy body – it is about making peace with the body you have now, and enabling it to naturally meet the demands of daily life, exercise, and the challenges that come your way.
If you have further questions, you are welcome to book a one-on-one assessment and consultation with us.

参考文献 References
1. Bezuhla, M., & Yudenko, O. (2023). Modern approaches to physical therapy of women with diastasis recti of the abdominal muscles as a result of multiple pregnancy. The Ukrainian Scientific Medical Youth Journal, 139(2), 40-49. https://doi.org/10.32345/USMYJ.2(139).2023.40-49
2. Huang, M., Huang, Z. & Huang, H. Precision medicine exploration of postpartum rectus abdominis muscle separation: from basic research to clinical practice. BMC Surg 25, 550 (2025). https://doi.org/10.1186/s12893-025-03285-x
3. Hernández-Granados P, Henriksen NA, Berrevoet F, Cuccurullo D, López-Cano M, Nienhuijs S, Ross D, Montgomery A. European Hernia Society guidelines on management of rectus diastasis. Br J Surg. 2021 Oct 23;108(10):1189-1191. doi: 10.1093/bjs/znab128. PMID: 34595502; PMCID: PMC10364860.
4. Luo X, Leng X, Jiang J. The relationship between transversus abdominis and rehabilitation exercises for diastasis recti abdominis: A scoping review. Journal of Bodywork and Movement Therapies, 2025; 45, 619-626
5. Beamish NF, Davenport MH, Ali MU, et al. Impact of postpartum exercise on pelvic floor disorders and diastasis recti abdominis: a systematic review and meta-analysis. British Journal of Sports Medicine 2025;59:562-575.
6. Bigdeli, N., Yalfani, A., Doosti-Irani, A. et al. An evidence-based comparison of rehabilitation strategies for diastasis recti abdominis in postpartum women: a systematic review and network meta-analysis. Sci Rep 15, 39591 (2025). https://doi.org/10.1038/s41598-025-22574-2
7. JANISZEWSKA, Michalina, FEJA, Ewa and ŁUCZAK, Janusz. Comprehensive management of diastasis recti abdominis after childbirth: a literature review. Journal of Education, Health and Sport. Online. 16 November 2025. Vol. 85, p. 66585. [Accessed 9 July 2026]. DOI 10.12775/JEHS.2025.85.66585.
8. Bracale, U., Stabilini, C., Cavallaro, G. et al. The Italian national consensus conference on the diagnosis and treatment of Rectus Abdominis diastasis in Post-gravidic Women. Hernia 29, 213 (2025). https://doi.org/10.1007/s10029-025-03403-x
9. Zhou, R., Mao, X., Hou, Y. et al. Optimizing Rectus Sheath Plication in Lipoabdominoplasty: Correlation Between Corrected Distance, Intra-abdominal Pressure and Postoperative Pain. Aesth Plast Surg 49, 6111–6119 (2025). https://doi.org/10.1007/s00266-025-05198-9
免责声明:本文观点为作者个人意见,不应视作个人医疗建议。提供的信息旨在帮助读者做出自身健康的知情决策。
Disclaimer: This article reflects the author’s professional opinion and is not a substitute for personal medical advice. The information provided is intended to help readers make informed decisions about their health.